

Proximal tib-fib stabilization using the cutting edge tightrope technique
Dr. Garcia specializes in complex knee, shoulder and elbow sports surgeries. He has prepared a number of surgical videos below to help patients better understand their procedures. He is frequently updating his surgical video database so check back soon for further updates.
This video, titled "Proximal tib-fib stabilization using the cutting edge tightrope technique," demonstrates a surgical solution for a relatively rare knee condition: chronic proximal tibiofibular (tib-fib) joint instability. This joint is where the shinbone (tibia) meets the smaller bone on the outside of the lower leg (fibula) just below the knee.
In this patient, the joint became visibly unstable and shifted out of place when the knee was bent (flexion) but naturally put itself back in place when the leg was straightened (extension). Because conservative treatment like temporary joint taping failed to resolve the symptoms, the surgeon utilized an innovative, minimally invasive approach using an Arthrex TightRope system—a high-strength suture-and-button device originally designed for severe ankle sprains.
The key aspects of the procedure include:
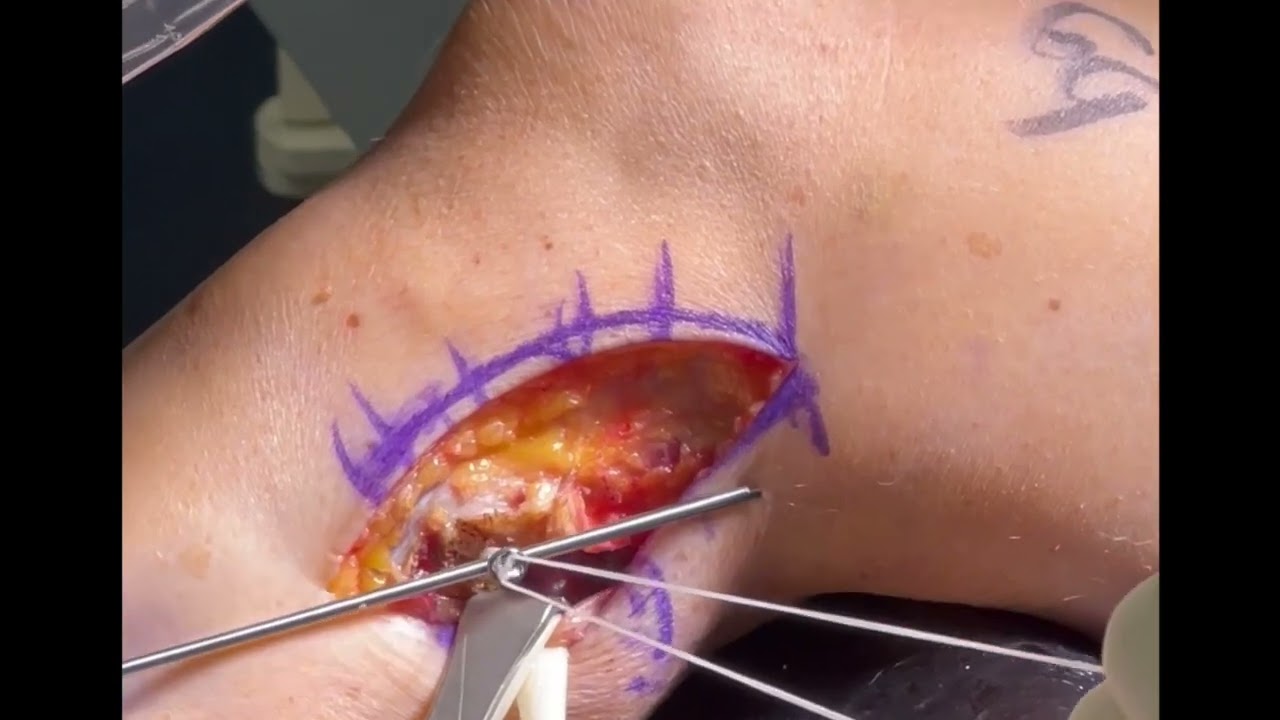
- Surgical Exposure and Critical Nerve Protection: The surgeon makes an incision on the outside of the knee to access the posterolateral corner. Because of the anatomy, the peroneal nerve (the major nerve responsible for lifting the foot) runs directly across the surgical area. The surgeon carefully dissects out and isolates this nerve so it can be physically protected from instruments throughout the entire operation.
- Fluoroscopic Tunnel Drilling: Using real-time X-ray (fluoroscopy) guidance, a guide wire is driven from the outside of the fibula straight through into the tibia. A drill is then passed along the wire to create a single tunnel through all four bone cortices (the hard outer walls of both bones).
- Deploying the TightRope Device: The tiny metallic button of the TightRope is fed through the tunnel until it exits the far inner side of the shinbone. The surgeon engages the device to flip the button flat, pulling it back until it rests securely flush against the inner bone wall of the tibia.
- Reduction and Final Tensioning: With the knee bent at a 90-degree angle, the surgeon pulls the heavy-duty suture tails to clamp the second button tightly against the outside of the fibula, compressing the loose joint back into its normal position. To ensure long-term stability, the knee is flexed and extended multiple times to work out any initial slack or "creep" in the sutures before a final tightening is performed.
- Anatomic Closure: After verifying that the dynamic instability is completely eliminated, the surgeon repairs the biceps femoris tissue back over the top of the hardware, making absolutely sure the peroneal nerve remains free from any pressure or impingement.
The surgeon highlights that this modern suture-button approach provides the same rigid stability as a traditional, highly invasive tendon reconstruction, but benefits the patient with a significantly faster recovery timeline and a quicker return to sports.







