

Dr. Garcia demonstrates his technique for acute elbow LCL repair
Dr. Garcia specializes in complex knee, shoulder and elbow sports surgeries. He has prepared a number of surgical videos below to help patients better understand their procedures. He is frequently updating his surgical video database so check back soon for further updates.
In this video, Dr. Grant H. Garcia demonstrates his surgical technique for an acute elbow lateral collateral ligament (LCL) repair, combined with an initial elbow arthroscopy. The patient suffered from significant rotatory instability following an acute fall less than four weeks prior.
Procedure Overview
- Initial Arthroscopy: Dr. Garcia begins with an arthroscopic evaluation of the elbow. No loose bodies are found in the radiocapitellar joint or anterior recess. However, a small amount of cartilage damage is noted on the capitellum, though it is not severe enough to require microfracture or further cartilage procedures.
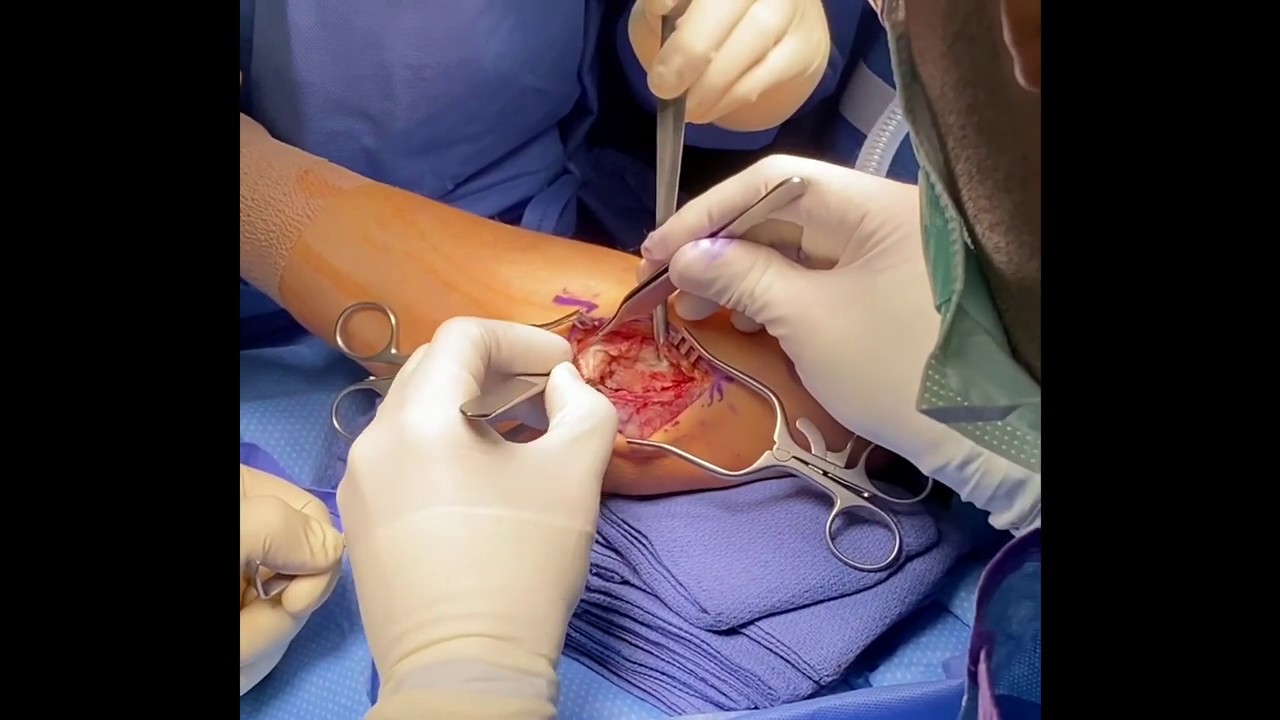
- Surgical Dissection & Exposure: A lateral-based incision is made, and dissection is carried down to the LCL. The lateral tissues are peeled back to evaluate the tear, which involves a combination of the radial collateral ligament and the lateral ulnar collateral ligament (LUCL). The edges are cleaned, and the fascial and muscular layers are released to isolate the ligament tissue. During this release, the arm is kept in pronation to protect the posterior interosseous nerve (PIN).
- Instability Assessment: An examination under anesthesia shows the severity of the injury. Upon full extension, the radiocapitellar joint completely dislocates, explaining the cartilage damage observed earlier during the arthroscopy.
- Anchor Placement: A single 4.75 mm corkscrew anchor with suture tape attached is placed at the isometric point of the capitellum to allow for an anatomic repair.
- Ligament Repair (Tension Slide Technique): A modified Krackow suture technique is used to secure the ligament tissue, ensuring the sutures do not bind up so the LCL can lay flat against the bone for optimal healing. With the arm positioned to apply appropriate compression, high-tensile suture tape is tied down using consecutive half-hitches. The major portion of the LCL complex is tied down and secured while holding the arm in supination to establish proper tension. These sutures are also saved to assist with closing the joint capsule later.
- Post-Repair Evaluation: A secondary examination under anesthesia confirms that the radiocapitellar joint is completely aligned, perfectly anatomic, and fully stable. The elbow moves smoothly with no catching or locking from the minor cartilage defect.
- Closure: The procedure concludes by using the remaining suture tape to repair the extensor muscles that were reflected during exposure, achieving a complete closure of the lateral side of the elbow.







