

Dr. Garcia demonstrates his Superior Capsular Reconstruction technique.
Dr. Garcia specializes in complex knee, shoulder and elbow sports surgeries. He has prepared a number of surgical videos below to help patients better understand their procedures. He is frequently updating his surgical video database so check back soon for further updates.
In this comprehensive surgical demonstration, Dr. Grant Garcia walks through a complex, revision Superior Capsular Reconstruction (SCR) technique on a patient with a massive, unrepairable retracted rotator cuff tear accompanied by an upper subscapularis tear.
The presentation details each key phase of the reconstruction:
- Subscapularis Repair: Because the upper subscapularis is torn and lifting off, Dr. Garcia first repairs it using an inverted horizontal mattress technique with a SwivelLock anchor. He preserves the stay stitches from this repair to help tie down the anterior aspect of the graft later.
- Joint Debridement and Preparation: The surgery requires extensive scar tissue release because it is a failed revision case. Dr. Garcia performs a subacromial decompression and clears old sutures and anchors. He then burs the superior glenoid down to a fresh, bleeding bony bed and uses a power pick to create small micro-fracture holes across the humeral footprint to enhance biological healing.
- Glenoid and Humeral Anchor Placement: Using a percutaneous guide system, Dr. Garcia inserts three knotless FiberTack anchors into the superior glenoid at roughly the 10, 12, and 2 o'clock positions. The anchors feature a 15-degree angle to prevent bone blowout. He then prepares the lateral row on the humerus for SwivelLock anchors, spacing them 20 to 25 millimeters apart.
- Graft Measurement and Preparation: Using a specialized SCR measuring device with the patient's arm abducted 30 to 40 degrees (ensuring the patch stays tight when the arm is resting at the side), Dr. Garcia calculates the exact distances between all anchors. He maps these coordinates onto a 3-millimeter thick dermal allograft, cuts it to shape, and punches holes only on the lateral edge where the heavy FiberTapes will pass through.
- Suture Management and Graft Introduction: The self-locking blue sutures from the glenoid are passed through the medial edge of the patch in a horizontal mattress fashion. After double-checking all lines to ensure absolutely zero suture entanglement, the large patch is carefully guided through a passport cannula using a Kingfisher tool and securely tensioned down to the glenoid bone.
- Lateral Row Fixation: Moving to the humerus, the FiberTapes are threaded into SwivelLock anchors. Dr. Garcia guides the anchors directly to the margin of the patch before deploying them into the bone, maximizing compression and eliminating all slack across the double-row construct.
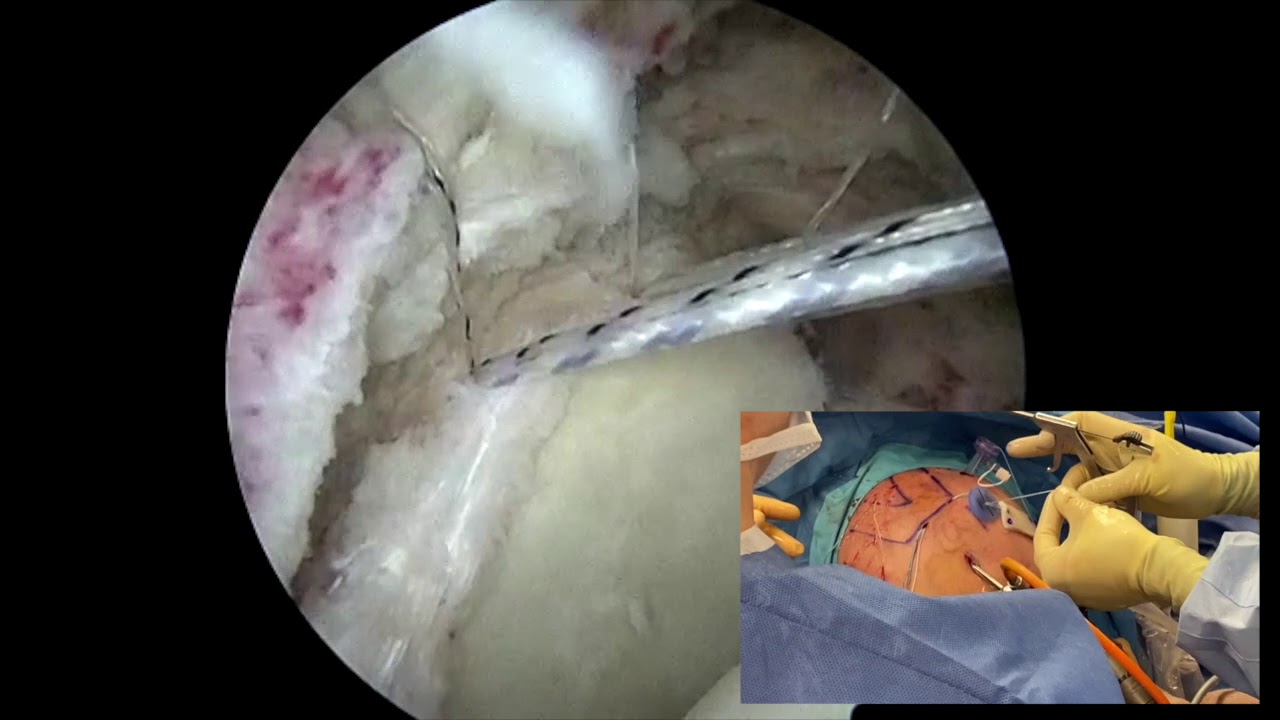
- Side-to-Side Margin Convergence: To fully recreate the superior capsule and minimize empty space, Dr. Garcia uses a Scorpion device to place interrupted fiber wire stitches. These stitches tie the posterior and remaining native rotator cuff directly to the edges of the newly implanted graft. The anterior edge is secured using the stay stitches from the initial subscapularis repair.
At the close of the procedure, a probe test from the lateral portal verifies the tight, "sucked-down" appearance of the graft. Manual superior pressure on the humeral head confirms excellent, multi-point stability with no superior migration or shifting.







