

Dr. Garcia demonstrates his innovated technique for partially torn, articular sided rotator cuff repairs.
Dr. Garcia specializes in complex knee, shoulder and elbow sports surgeries. He has prepared a number of surgical videos below to help patients better understand their procedures. He is frequently updating his surgical video database so check back soon for further updates.
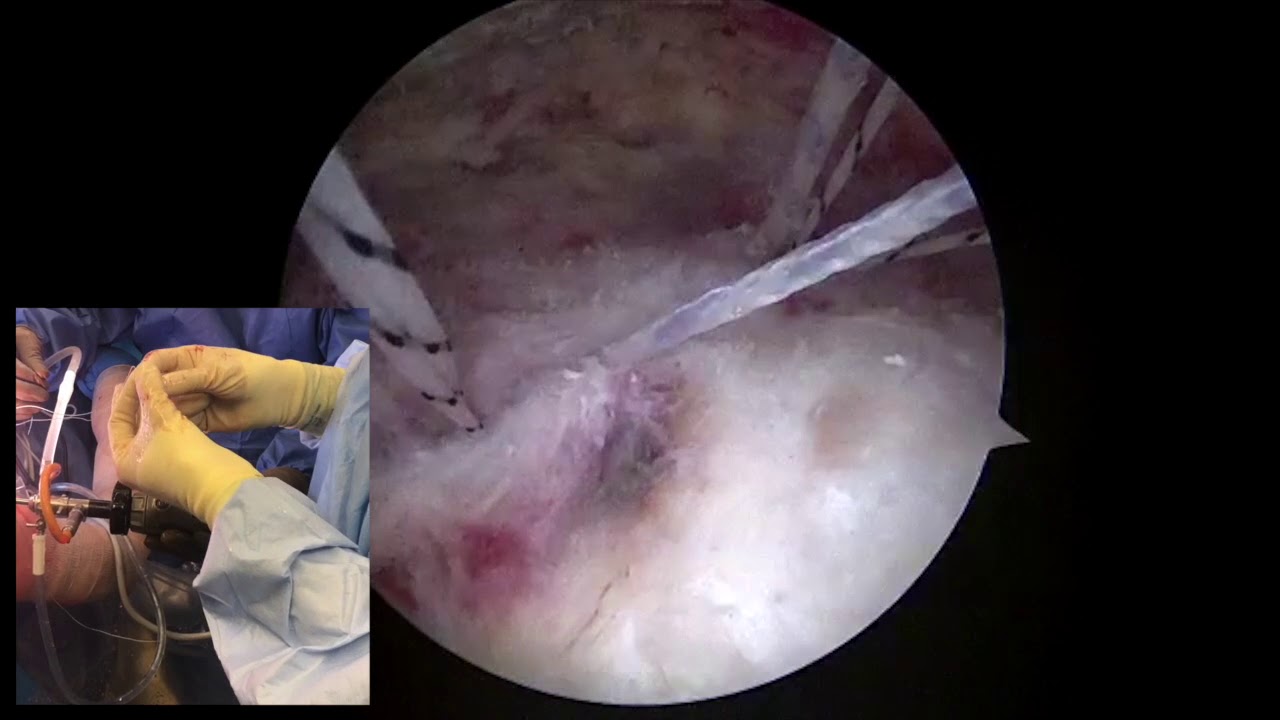

In this surgical presentation, Dr. Grant Garcia demonstrates an innovative, percutaneous technique for repairing a PASTA tear (Partial Articular Surface Tendon Avulsion), which is a partially torn, articular-sided rotator cuff tear. Because the outer (bursal) side of the rotator cuff remains completely healthy and intact, this specialized arthroscopic method allows the surgeon to repair the deep, damaged side without cutting through or sacrificing the intact external tissue.
The video highlights the key steps of this percutaneous repair:
- Articular Debridement: Using an arthroscopic shaver, Dr. Garcia cleans and prepares the torn, articular-sided bony bed of the humerus. This removes damaged tissue and creates a fresh surface optimized for bone-to-tendon healing.
- Percutaneous Anchor Placement: To minimize trauma to the healthy tissue, a spinal needle and wire system are used to percutaneously pierce through the intact outer cuff. A cannulated dilator gently splits the tissue fibers, allowing the surgeon to insert a 3.9 mm knotless anchor into the bone at the anterior margin of the tear. This exact process is repeated to place a second knotless anchor at the posterior margin.
- Subacromial Decompression: To protect the suture lines, temporary "fiber sticks" are placed in the subacromial space. Dr. Garcia shifts the camera to the bursal side to perform a debridement of the thickened bursa and a mild acromioplasty (shaving a small amount of bone off the underside of the acromion). This flat surface prevents future mechanical pinching or impingement.
- Knotless Suture Shuttling: Back inside the joint, the specialized knotless loop mechanism is activated. The blue main suture from the posterior anchor is threaded into the loop of the anterior anchor and shuttled through, creating an internal bridge across the tear. The main suture from the anterior anchor is similarly shuttled back through the posterior anchor's loop.Tensioning and Compression: Under direct visualization, the surgeon carefully cinches down both suture lines simultaneously. This pulls the deep, detached portion of the rotator cuff tightly back down against its bony footprint, achieving maximum articular compression.
- Tensioning and Compression: Under direct visualization, the surgeon carefully cinches down both suture lines simultaneously. This pulls the deep, detached portion of the rotator cuff tightly back down against its bony footprint, achieving maximum articular compression.
- Lateral Row Fixation: To secure the construct externally without tying knots, the remaining suture tails are brought out to the lateral side of the humerus. They are inserted into a 4.75 mm PushLock anchor, providing a final layer of flat, low-profile compression on the bursal surface.
This double-row, knotless technique effectively treats the articular detachment while completely preserving the structural integrity of the healthy, uninjured portion of the rotator cuff.







