

Dr. Garcia demonstrates his cutting edge technique for subscapularis repair after stemless total shoulder replacement.
Dr. Garcia specializes in complex knee, shoulder and elbow sports surgeries. He has prepared a number of surgical videos below to help patients better understand their procedures. He is frequently updating his surgical video database so check back soon for further updates.

In this video, Dr. Grant Garcia demonstrates his cutting-edge, double-row transosseous subscapularis repair technique following a stemless total shoulder replacement. This approach provides vastly superior strength over a traditional single-row repair and offers an extra layer of fixation by securing the construct directly around the implant's internal components.
The demonstration outlines the core stages of the surgical technique:
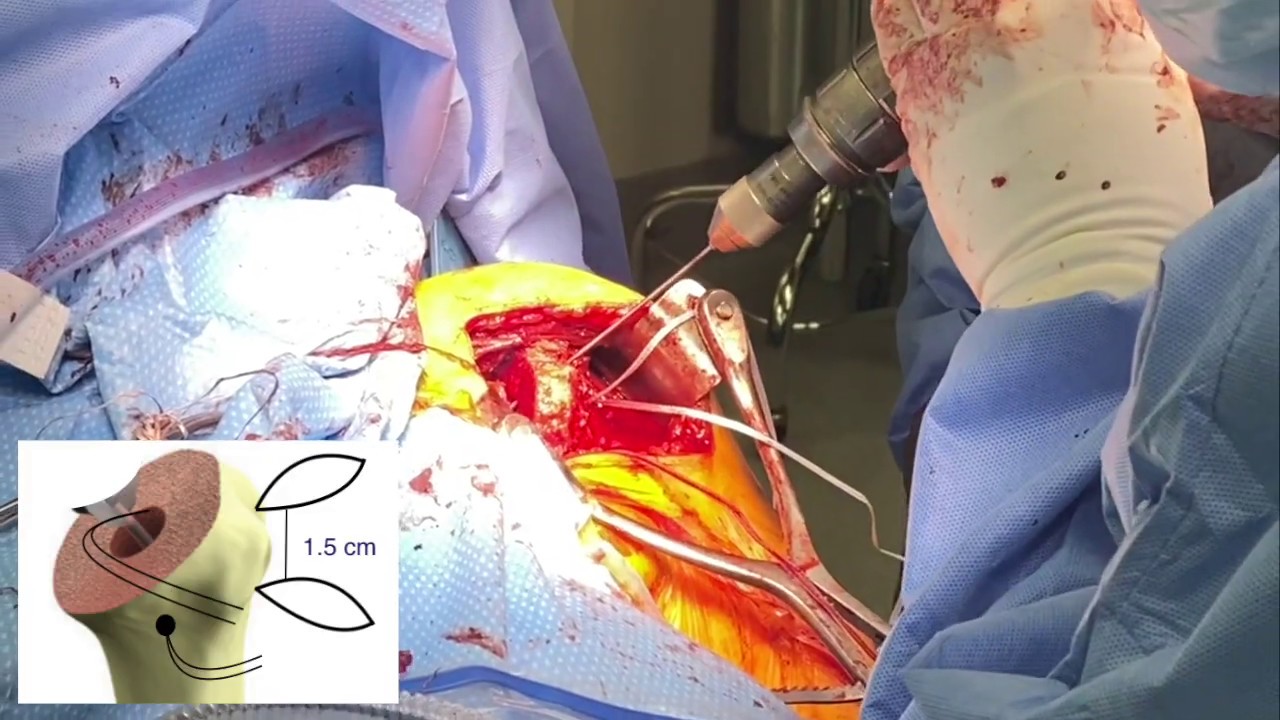
- Drilling and Initial FiberTape Placement: Using a 2.0 mm drill, the surgeon creates a tunnel through the lateral portion of the bicipital groove. A heavy FiberTape suture is passed through the tunnel and channeled beneath the lesser tuberosity into the central canal. A second, identical FiberTape is placed through a separate tunnel drilled roughly 1.5 centimeters superior (higher) to the first.
- The Cinch Knot Mechanism: The higher, superior FiberTape is designated to go around the trunnion (the neck component) of the stemless replacement. Dr. Garcia uses a marking pen to carefully track the corresponding limbs. He applies a specialized loop cinch knot, holding it tightly against the lateral bone cortex using an arthroscopic grasper to ensure all slack is completely eliminated.
- Seating the Implant Component: The base plate of the stemless implant is mounted while maintaining strict tension on both lateral FiberTapes. The upper suture loops cleanly over the base plate without blocking the trunnion hole. The humeral head component is manually fitted onto the trunnion and fully impacted into place, locking the superior suture cinch beneath it.
- Medial Row Tissue Passing: The four limbs of the medial fiber tapes are sequentially passed through the subscapularis tendon using a suture passer. The upper limbs are threaded roughly 1 to 1.5 centimeters medial to the remaining tendon edge. This layout is meticulously tracked to set up a robust, crisscross double-row arrangement.
- Final Suture Tensioning and Knot Tying: With the patient's arm positioned in abduction and maximum internal rotation, the corresponding limbs from the upper and lower fiber tapes are pulled back through the cinch knots using a loop grasper. Dr. Garcia secures the tendon to the bone by tying alternating half-hitches over the cinch mechanisms, achieving highly rigid, flat compression.
- Rotator Interval Closure: To conclude the anatomical reconstruction, a separate suture tape is used to close the rotator interval in a figure-eight fashion. This re-establishes the natural connection between the supraspinatus and subscapularis muscles, providing a final safeguard against a postoperative subscapularis rupture.







