

Dr. Grant Garcia specializes in MQTFL (Medial Quadriceps Tendon Femoral Ligament) reconstruction, an advanced procedure used to treat recurrent patellar instability and kneecap dislocations. This technique helps restore stability while minimizing the risk of complications associated with traditional fixation methods. Patients in Seattle, Bellevue, Everett, and Kirkland, WA, receive personalized care focused on improving knee function, reducing instability, and supporting a safe return to sports and daily activities.
Background:
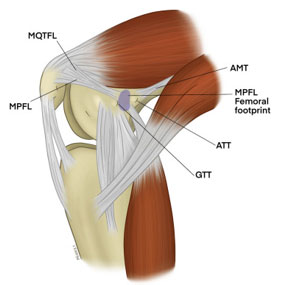
Medial quadriceps tendon femoral ligament (MQTFL) reconstruction is a surgical procedure indicated in patients with more severe patellar instability. Medial quadriceps tendon femoral ligament is a band of tissue that extends from the femur to the quadriceps insertion at the patella. Medial quadriceps tendon femoral ligament is the major ligament which stabilizes the patella and helps in preventing patellar subluxation (partial dislocation) or dislocation. This ligament can rupture or get damaged when there is patellar lateral dislocation. Dislocation can be caused by direct blow to the knee, twisting injury to the lower leg, strong muscle contraction, or because of a congenital abnormality such as shallow or malformed joint surfaces.
Medial quadriceps tendon femoral ligament reconstruction using tissue grafts is done by sfollowing the basic principles of ligament reconstruction such as:
- Graft Selection: Strong and stiff graft should be selected
- Location: The graft should be located isometrically
- Correct tension: The tension set in the graft should be appropriate
- Secure Fixation: Stable fixation of the graft should be achieved
Surgical Technique
Check out my technique for MQTFL reconstruction. This can be used for kneecap dislocation or patients that undergo patellofemoral replacement.

An incision is made on the inner aspect of the knee and a socket is drilled at the origin of the medial quadriceps tendon femoral ligament on the femur. A graft is docked in the socket and fixed with a screw. Then the graft is tunneled under the soft tissue to another incision made over the quadriceps insertion on the patella. The graft is then woven into the quadriceps tendon and folded back to itself and secured with high-tension sutures. The soft tissues are closed and a dressing is applied.
Benefits of this technique:
This technique reduces drilling into the patella which can have a slightly higher risk of fracture etc. In addition, it can be a good alternative in younger patients with open growth plates to avoid drilling into the patella growth plates or in patients with previous hardware in the patella with continued instability. Finally, another good alternative use for this is in patient with previous patella replacement, either patellofemoral replacement or total knee replacement, who have continued recurrent instability of the patella. Dr. Garcia is one of the few surgeons in the state of Washington that performs this procedure.
Post-operative care
Rehabilitation exercises are initiated for range of motion, strength, and endurance. Return to full activities is usually 5-6 months after surgery. Success rates are high with no recurrent dislocations as high as 90-95% in long term studies.







