

Dr. Grant Garcia specializes in glenoid fracture repair and fixation for patients who have sustained shoulder socket fractures due to trauma or dislocation injuries. These complex injuries can lead to pain, instability, and long-term dysfunction if not properly treated. Patients in Seattle, Bellevue, Everett, and Kirkland, WA, receive advanced, personalized care focused on restoring shoulder alignment, stability, and optimal joint function.
Dr. Garcia utilizes the newest arthroscopic techniques for glenoid fracture repair and fixation, allowing for precise reduction of fracture fragments with minimal soft tissue disruption. This minimally invasive approach enhances visualization, improves fixation accuracy, and supports faster recovery. By restoring the anatomy of the shoulder socket, this technique helps improve stability, reduce pain, and promote long-term functional outcomes for patients.
Dr.Garcia’s newest technique for arthroscopic glenoid fracture repair
Analysis of NFL Quarterback Deshaun Watson's Injury
Background:
The glenoid is the socket part of the ball-and-socket shoulder joint. It's part of the scapula (shoulder blade), which is a thin, broad bone that sits behind the rib cage. The scapula itself is mobile (its orientation shifts on your back with movement), and normal scapular motion is important for normal shoulder function.
The glenoid is the socket part of the ball-and-socket shoulder joint. It's part of the scapula (shoulder blade), which is a thin, broad bone that sits behind the rib cage. The scapula itself is mobile (its orientation shifts on your back with movement), and normal scapular motion is important for normal shoulder function.
To make it a little deeper, another type of cartilage called the shoulder labrum surrounds the glenoid. When there's a problem with the labrum, the shoulder is prone to episodes of shoulder instability, such as dislocation. This often occurs when people tear the shoulder labrum.
Indications
Understanding if you have a glenoid fracture may not be obvious at first. Common indicators include:
- Intense pain in the shoulder following trauma
- Difficulty or inability to move the arm
- Swelling and bruising around the shoulder area
- Visible deformity or an unusual shoulder shape
Types
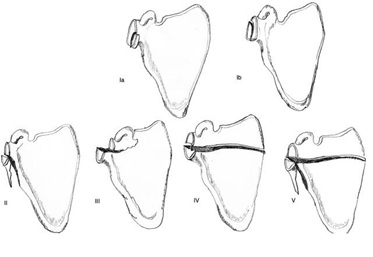 Fractures of the glenoid are a relatively uncommon type of shoulder fracture, only accounting for about 10%. Glenoid fractures most often occur when there is significant trauma to the shoulder, or because of high-energy sports injuries.
Fractures of the glenoid are a relatively uncommon type of shoulder fracture, only accounting for about 10%. Glenoid fractures most often occur when there is significant trauma to the shoulder, or because of high-energy sports injuries.
The two most common fracture patterns are:
- Glenoid Lip Fractures: Glenoid lip fractures occur when there is a shoulder dislocation or shoulder subluxation, and the ball comes out of the socket. As the ball dislocates, it can push against the rim of the glenoid socket, causing a fragment of the bone to fracture. Treatment of a glenoid rim fracture is focused on restoring the normal contour of the shoulder socket to prevent recurrent instability (repeat dislocations) of the shoulder joint. Surgical treatment is often considered for these injuries, especially when the fracture is out of position or if there is a large fragment of the glenoid bone.
- Glenoid Fossa Fractures: The glenoid fossa is the center portion of the socket. Glenoid fossa fractures are much less common injuries, and often associated with severe trauma. There is little data on the ideal treatment of these injuries because they are so uncommon. However, most surgeons agree that fracture management decisions must consider both the fracture type and the patient's need. More active patients with fractures that are not in the proper position will most likely benefit from surgery to realign these injuries.
Workup and Planning
After an injury, a thorough examination and imaging studies, like X-rays and CT scans, are essential. These allow for:
- Proper classification of the fracture.
- Assessment of associated injuries.
- Formulating a management plan tailored to the patient.
Treatment
Dr. Garcia demonstrates his Arthroscopic Glenoid Repair Technique
In general, it is agreed that unstable fractures are best treated with surgery whereas stable fractures can be treated conservatively. The goal of surgical treatment is to restore the alignment of the normal joint surface. It is typical to repair the bone with small plates and/or screws to ensure that the bones heal in the proper position. New arthroscopic methods are available for glenoid fractures. These can be done with small poke holes and in most cases only suture anchors are required for healing.
Surgery Recommendations
Not all glenoid fractures require surgery. The decision depends on:
- The type and extent of the fracture.
- The degree of displacement.
- Patient’s age, activity level, and overall health.
Generally, non-displaced fractures (Type I) are managed without surgery, while displaced fractures often necessitate surgical intervention for optimal outcomes.
Arthroscopic Fixation
New arthroscopic methods are available for glenoid fractures. These can be done with small poke holes and in most cases only suture anchors are required for healing. This minimally invasive procedure employs small incisions and specialized instruments. Benefits include:
- Less post-operative pain.
- Faster recovery.
- Reduced risk of complications.
During the procedure, the surgeon uses an arthroscope (a tiny camera) to visualize the fracture and guide small instruments to fix the broken fragments using anchors, suture or screws if needed.
Surgical Outcomes
With advances in orthopedic surgery, outcomes for glenoid fractures are promising. However, the result largely depends on:
- The severity of the fracture.
- The expertise of the surgeon.
- Patient’s adherence to post-operative care and physiotherapy.
Many patients regain good shoulder function post-recovery. However, potential complications can include:
- Limited range of motion.
- Chronic pain.
- Arthritis of the shoulder.
It's essential to have regular follow-ups with your orthopedic surgeon to monitor healing and ensure an optimal recovery trajectory.
Rehabilitation:
Rehabilitation after surgery to repair a glenoid fracture is focused on restoring normal mobility and strength to the shoulder joint. Your surgeon may recommend a brief time of immobilization to allow the bones to begin to heal, but as soon as possible will begin range-of-motion exercises. As the healing becomes stronger, you will progress to strengthening exercises of the shoulder.
Risks of Surgery:
Risks of surgical treatment include infection, shoulder stiffness, nerve injury, and shoulder arthritis. The reason people may develop arthritis of the joint is because of the trauma to the cartilage surface of the socket. Even if surgery is performed to realign the damaged bone, the injury to the cartilage increases the chance of the development of arthritis, which in turn increases the risk of shoulder replacement surgery later in life.
Conclusion
Glenoid fractures, though complex, have a good prognosis when managed appropriately. Understanding the nature of the injury, available treatment options, and potential outcomes empowers patients to make informed decisions about their care.







