

AC Joint Separation
Dr. Grant Garcia specializes in the treatment of AC joint separations, injuries that occur when the ligaments connecting the collarbone to the shoulder blade are damaged or torn. Commonly caused by sports injuries, falls, or direct trauma, AC joint separations can result in pain, swelling, and instability. Patients in Seattle, Bellevue, Everett, and Kirkland, WA, receive personalized care focused on restoring shoulder function and relieving discomfort.
AC Joint injury,shoulder separation , treatment - Everything You Need To Know - Dr. Nabil Ebraheim
Content from orthobullets.com
Background:
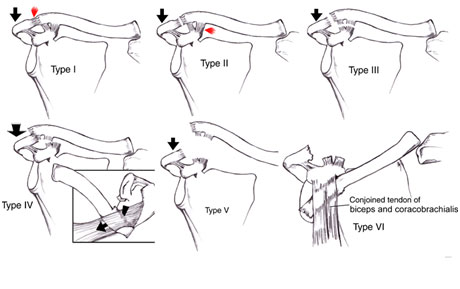
- an acromioclavicular joint injury, otherwise known as a shoulder separation, is a traumatic injury to the acromioclavicular (AC) joint with disruption of the acromioclavicular ligaments and/or coracoclavicular (CC) ligaments
- treatment is immobilization or surgical reconstruction depending on the degree of separation and ligament injury.
- incidence
- common injury making up 9% of shoulder girdle injuries
- demographics
- more common in males and athletes
- mechanism
- direct blow to the shoulder
- often sustained while falling onto the shoulder
Epidemiology
Pathophysiology
Dr. Garcia demonstrates his cutting edge technique for revision AC reconstruction surgery
Anatomy:
- Stability
- static
- joint capsule
- acromioclavicular (AC) ligaments
- controls horizontal motion and anterior-posterior stability
- has superior, inferior, anterior and posterior components
- posterior and superior AC ligaments are most important for stability
- coracoclavicular (CC) ligaments
- controls vertical motion and superior-inferior stability
- two ligaments
- conoid
- medial
- inserts on clavicle 4.5cm medial to lateral edge
- most important for vertical stability
- trapezoid
- lateral
- inserts on clavicle 3cm medial to lateral edge
- conoid
- dynamic
- anterior deltoid
- trapezius
- static
Presentation:
- Symptoms
- pain
- usually over AC joint
- can also be referred to the trapezius
- pain
- Physical exam
- lateral clavicle or AC joint tenderness
- abnormal contour of the shoulder compared to contralateral side
- stability assessment
- horizontal (anterior-posterior) stability evaluates AC ligaments
- cross-body adduction
- horizontal instability (ISAKOS type 3B) may indicate need for more aggressive treatment
- vertical (superior-inferior) stability evaluates CC ligaments
- horizontal (anterior-posterior) stability evaluates AC ligaments
Check out Dr. Garcia’s minimally invasive and arthroscopic assisted AC joint reconstruction.
Treatment Options:
- Nonoperative
- brief sling immobilization, rest, ice, physical therapy
- indications
- type I and II
- type III in most individuals
- good results when clavicle displaced < 2cm
- rehab
- early shoulder range of motion
- regain functional motion by 6 weeks
- return to normal activity at 12 weeks
- consider corticosteroid injections
- outcomes
- type III treated non-op had higher DASH scores at 6 weeks and 3 months, and equal function at 1 year with lower rate of secondary surgery (removal of hardware) compared to those treated operatively
- complications
- AC joint arthritis
- chronic subluxation and instability
- indications
- brief sling immobilization, rest, ice, physical therapy
Check out Dr. Garcia’s new innovative technique for AC joint reconstruction.
Operative
- CC interval restoration (ORIF vs. Ligament Reconstruction)
- indications
- acute type IV, V or VI injuries
- recent studies suggest no difference in functional outcomes between operative and nonoperative interventions for high grade injuries
- acute type III injuries in laborers, elite athletes, patients with cosmetic concerns
- chronic type III injuries that failed non-op treatment
- historically it was thought acute injuries were treated with ORIF and chronic injuries were treated with CC ligment reconstruction
- however, new studies have shown no difference in outcomes in types III injuries treated surgically after 6 weeks non-op treatment versus immediate surgery
- historically it was thought acute injuries were treated with ORIF and chronic injuries were treated with CC ligment reconstruction
- acute type IV, V or VI injuries
- contraindications
- patient unlikely to comply with postoperative rehabilitation
- skin problems over fixation approach site
- techniques
- ligament reconstruction with soft tissue graft
- Modified Weaver-Dunn
- distal clavicle excision with transfer of coracoacromial ligament to the distal clavicle to recreate CC ligament
- autograft
- allograft
- Modified Weaver-Dunn
- fixation
- suture
- hook plate
- CC screw (Bosworth)
- cortical flip button (e.g Dog Bone)(+/- arthroscopic assistance)
- K-wire
- ligament reconstruction with soft tissue graft
- rehabilitation
- sling immobilization for 6 weeks, no shoulder range of motion
- return to full activity after 6 months
- indications
For more information visit orthobullets.com







